+ 82-2-2088-4921
bmkhalo@gmail.com
하남시 조정대로 150
(우) 12930
Mon - Fri
09h - 18h
MSE


INVENTED BY Prof. WON MOON
INVENTED BY Prof. WON MOON
UCLA School of Dentistry, Certificate in Orthodontics, 1991
UCLA School of Dentistry, MS in Oral Biology, 1991
Harvard School of Dental Medicine, D.M.D., 1989
University of California, Irvine, BS in Mathematics, 1984
MSE Lab Works
1. MSE Position: Posterior Palatal Vault Between 1st and 2nd Molars in Order to Direct the Expansion Force Against the Buttress Bones.
2. MSE Should Be Positioned Slightly Anterior to the Soft Palate
Bi-Cortical Engagement

Benefits & Contraindications
Benefits
Vertical Control in High Angle Cases
Significant Increase in Upper Airway Volume: Nasal Obstruction, Sleep Apnea
Mostly Skeletal Expansion: Less Bone Bending and Dental Tipping Compared to RPE and SARPE
Less Invasive than SARPE and Orthognathic Surgery
FM and MSE for Class III Correction
MSE Causes Expansion of the Surrounding Structures
MSE Can Be Used for Mature Patients
Contraindications
Extremely narrow palatal vault
Patients with previous mid-facial trauma
Extremely thick/dense palatal bone and/or dense buttress bone
Extremely thin palate with low bone density
Activation Protocol
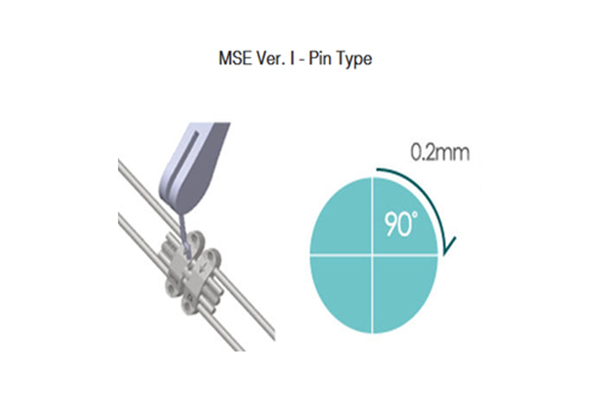
4 Turns = 0.8mm(1 revolution)
Ex) MSE-8 means its expansion size is 8mm = 40 turns
MSE Ⅰ
Early teens :3 turns / week(0.60mm /week)
Late teens :1 turns / day(0.20mm /day)
Early to Mid-20’s: 2~3 turns / day(0.40~0.60mm/day)
Older :Minimum 2~3 turns /day, assistance PRN
After Diastema : 1 turns / day(0.20mm / Day)
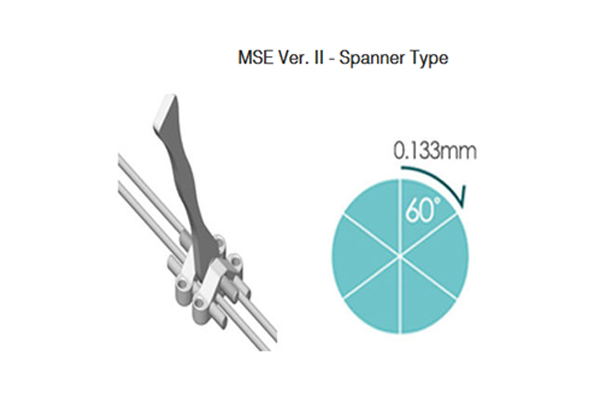
6 Turns = 0.8mm(1 revolution)
Ex) MSEⅡ-12 means its expansion size is 12mm = 90 turns
MSE Ⅱ
Early teens :6 turns / week(0.80mm /week)
Late teens :2 turns / day(0.27mm /day)
Early to Mid-20’s: 4~6 turns / day(0.53~0.80mm/day)
Older :Minimum 4~6 turns /day
After Diastema : 2 turns / day(0.27mm / Day)
History of MSE

MSE ver.1
MSE ver.2
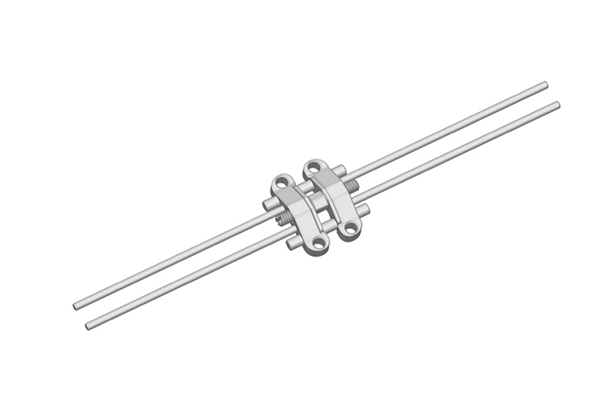
Specification


MSE mini implant

Clinical cases
<CASE 1: 19Y Male >

<CASE 2: adult>

<CASE 3: young adult>
